。曾經HA secrets 有一篇講到藥劑師係health care system上的重要性,奈何香港唔搞醫藥分家,藥劑師ge收入唔可以單靠dispense維生。
。衍生ge問題多,好似上次HEP. B出事,幫病人出藥之前藥劑師可以check返藥單,減低drug-related problem (DRP).
。提高藥劑師地位,其中一個就係醫藥分家。好簡單咁講,醫生要寫prescription,經藥劑師counsel之後出藥。好處係double-secure,但係分薄左醫生ge收入,當然唔會搞。
---不定時更新---
。其中一個藥劑師的責任就係medication reviews (e.g. HMR, RMMR),到底抵唔抵玩?
。如果搞,到底香港做唔做到醫藥分家?藥劑師的人工,時間,大眾印象,competency... etc
。藥劑師的counselling問題。聽醫生講定藥劑師講?聽病理學定應用藥理學?
。Pharmacy school 教出黎的野到底可不可以sustain?
[討論]點睇藥劑師
切柒奇俠
205 回覆
21 Like
3 Dislike
咁岩毓民又講醫療問題
係開始討論之前,先講講自己立場。
個人認為當初藥劑師係仲有市場,不過呢D都係理論上的問題,但係隨著科技的發展(尤其睇完上年AlphaGo點樣打贏Lee Sedol),呢行好快變成夕陽工業 。
。
個人認為當初藥劑師係仲有市場,不過呢D都係理論上的問題,但係隨著科技的發展(尤其睇完上年AlphaGo點樣打贏Lee Sedol),呢行好快變成夕陽工業
。Adverse drug events
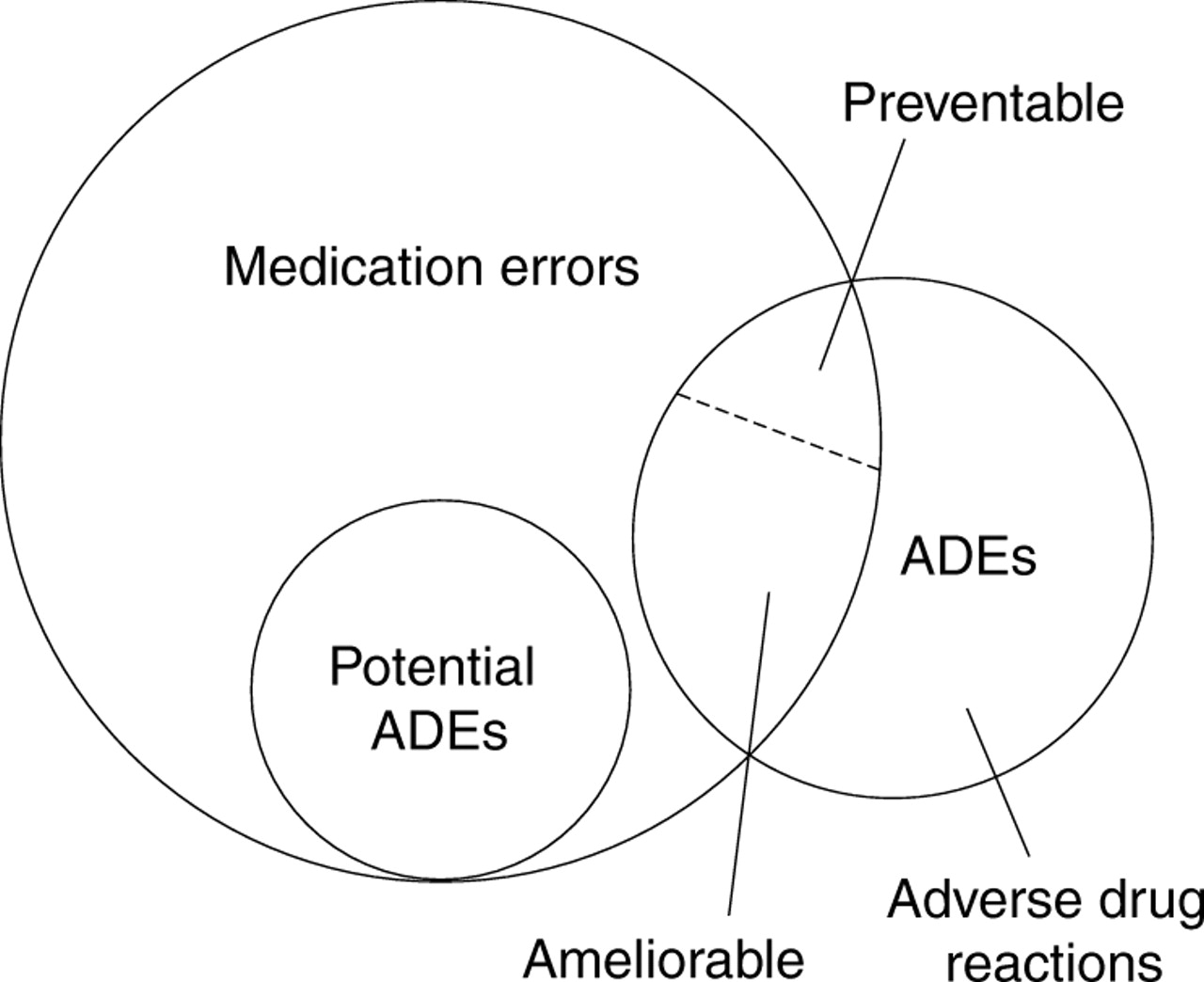
食藥就係為左醫病(/或者控制病情),但係有因應好多因素好似劑量或者基因,藥物GE副作用就會因應呢D因素而變大。好似長期痛症搞到要定時食止痛藥 Celebrex,雖然呢隻藥比起相近的止痛藥ibuprofen 冇咁傷胃,但係食耐左就會有更高心臟病風險,因此個ADE就係心臟病。
詳細mode of action唔會講,但係呢個例子想講ge係如果病人本身個體質唔適合食Celebrex ,到底醫生diagnosis 果陣會唔會考慮得咁仔細?唔係質疑緊醫生勁定廢,即係咁,你去一次公立醫院比較下輪候時間VS診症時間就知。
雖然呢個ADE係 preventable/ameliorable,但係有咩方法去降低個風險?教育?藥劑師COUNSEL去SHARE個WORKLOAD?
食藥就係為左醫病(/或者控制病情),但係有因應好多因素好似劑量或者基因,藥物GE副作用就會因應呢D因素而變大。好似長期痛症搞到要定時食止痛藥 Celebrex,雖然呢隻藥比起相近的止痛藥ibuprofen 冇咁傷胃,但係食耐左就會有更高心臟病風險,因此個ADE就係心臟病。
詳細mode of action唔會講,但係呢個例子想講ge係如果病人本身個體質唔適合食Celebrex ,到底醫生diagnosis 果陣會唔會考慮得咁仔細?唔係質疑緊醫生勁定廢,即係咁,你去一次公立醫院比較下輪候時間VS診症時間就知。
雖然呢個ADE係 preventable/ameliorable,但係有咩方法去降低個風險?教育?藥劑師COUNSEL去SHARE個WORKLOAD?
Pharmacist-led intervention
所以為左減低食錯藥ge問題,就出現左 pharmacist intervention.
就咁係Pubmed, 到搵 pharmacist intervention 已經有3223個items. 老實講,TL;DR。所以我搵幾個best match 出黎一齊睇。
——————
[1]Effect of critical care pharmacist's intervention on medication errors: A systematic review and meta-analysis of observational studies
The present systematic review and meta-analysis did not demonstrate a significant beneficial effect of the intervention on general MEs. However, the pooled analysis supported the role of pharmacists in reducing preventable ADEs and prescribing errors. Future high-quality studies that examine the effect of a critical care pharmacist are warranted.
[2]Effect of pharmacist intervention on physician prescribing in patients with chronic schizophrenia: a descriptive pre/post study
Results
a.) the dose and the number of antipsychotics at 1 year were significantly lower post-intervention.
b.) The seclusion room use rate was not significantly different but tended to be lower post-intervention than pre-intervention.
c.) The cost for all medicines, antipsychotics, and psychotropics were significantly lower post-intervention than pre-intervention.
結論?
Pharmacist intervention has the potential to optimize medication prescribing and reduce medication costs in patients with chronic schizophrenia. It might be suggested ... consider the pharmacists’ ability to rationalize medication therapy in schizophrenia.
所以為左減低食錯藥ge問題,就出現左 pharmacist intervention.
就咁係Pubmed, 到搵 pharmacist intervention 已經有3223個items. 老實講,TL;DR。所以我搵幾個best match 出黎一齊睇。
——————
[1]Effect of critical care pharmacist's intervention on medication errors: A systematic review and meta-analysis of observational studies
The present systematic review and meta-analysis did not demonstrate a significant beneficial effect of the intervention on general MEs. However, the pooled analysis supported the role of pharmacists in reducing preventable ADEs and prescribing errors. Future high-quality studies that examine the effect of a critical care pharmacist are warranted.
[2]Effect of pharmacist intervention on physician prescribing in patients with chronic schizophrenia: a descriptive pre/post study
Results
a.) the dose and the number of antipsychotics at 1 year were significantly lower post-intervention.
b.) The seclusion room use rate was not significantly different but tended to be lower post-intervention than pre-intervention.
c.) The cost for all medicines, antipsychotics, and psychotropics were significantly lower post-intervention than pre-intervention.
結論?
Pharmacist intervention has the potential to optimize medication prescribing and reduce medication costs in patients with chronic schizophrenia. It might be suggested ... consider the pharmacists’ ability to rationalize medication therapy in schizophrenia.
諗住搵多幾篇黎睇,不過第一份好似已經夠做。
藥劑師的確係可以減低medical errors, 但係作用不大
藥劑師的確係可以減低medical errors, 但係作用不大
睇多少少,打埋醫藥分家就瞓,聽日再打
醫藥分家 - 1
醫生diagnosis, 藥劑師睇下隻藥食唔食得死你,童話一般ge故事,唔俾埋單俾錢。講之前首先睇下一個小研究
A comparison of medical and pharmacy students' knowledge and skills of pharmacology and pharmacotherapy.
一個研究比較緊醫/藥學生對藥理同藥療GE技術同認識
All medical and pharmacy students actively studying during 2 academic years, 2010 and 2011, were asked to complete the test during an interdisciplinary scheduled lecture hour during a mandatory 1 week course. To gain access to courses, students normally have to enrol in an online registration system Osiris.
TL;DR
1) Pharmacy students have better knowledge of basic pharmacology, but not of the application of pharmacology knowledge , than medical students, whereas medical students are better at writing prescriptions. Professional differences in knowledge and skills therefore might well stem from their undergraduate education .
醫生diagnosis, 藥劑師睇下隻藥食唔食得死你,童話一般ge故事,唔俾埋單俾錢。講之前首先睇下一個小研究
A comparison of medical and pharmacy students' knowledge and skills of pharmacology and pharmacotherapy.
一個研究比較緊醫/藥學生對藥理同藥療GE技術同認識
All medical and pharmacy students actively studying during 2 academic years, 2010 and 2011, were asked to complete the test during an interdisciplinary scheduled lecture hour during a mandatory 1 week course. To gain access to courses, students normally have to enrol in an online registration system Osiris.
TL;DR
1) Pharmacy students have better knowledge of basic pharmacology, but not of the application of pharmacology knowledge
, than medical students, whereas medical students are better at writing prescriptions. Professional differences in knowledge and skills therefore might well stem from their undergraduate education .醫藥分家 - 2
醫藥分家呢個concept 已經唔係第一日ge事,不如睇下其他國家先例先。
[1]Influence of the Separation of Prescription and Dispensation of Medicine on Its Cost in Japanese Prefectures
Thus, the separation system was as effective in reducing medicine costs as the use of generic medicines. Because of its medical economic efficiency, the separation system should be expanded, especially in Asian countries in which the system is underdeveloped.
呢度解釋下咩叫
Generic medicine containing the same active ingredient can be manufactured and sold by other companies once the patent for the existing brand has expired.
最重要係generic medicine 係平好多
...The economic effects of the separation system have rarely been studied with quantitative data because it is difficult to precisely compare the objects under study. ...
...frequent changes in the Japanese insurance system, it is difficult to evaluate the exact effect of each factor on medicine costs...
...medical expenses tend to increase as people age....
...We observed a significant negative correlation for the relationship between expansion of the separation system and medicine costs. This finding indicates that the separation system in Japan might reduce daily medicine costs...
...enables doctors to refrain from prescribing specific medicines, as they are no longer personally interested in drug-related profit margins for their institutions or themselves....
...The magnitude of the partial correlation coefficient for the generic medicine replacement ratio was similar to that of the expansion rate....
記住呢個study地點係日本
醫藥分家呢個concept 已經唔係第一日ge事,不如睇下其他國家先例先。
[1]Influence of the Separation of Prescription and Dispensation of Medicine on Its Cost in Japanese Prefectures
Thus, the separation system was as effective in reducing medicine costs as the use of generic medicines. Because of its medical economic efficiency, the separation system should be expanded, especially in Asian countries in which the system is underdeveloped.
呢度解釋下咩叫
Generic medicine containing the same active ingredient can be manufactured and sold by other companies once the patent for the existing brand has expired.
最重要係generic medicine 係平好多
...The economic effects of the separation system have rarely been studied with quantitative data because it is difficult to precisely compare the objects under study. ...
...frequent changes in the Japanese insurance system, it is difficult to evaluate the exact effect of each factor on medicine costs...
...medical expenses tend to increase as people age....
...We observed a significant negative correlation for the relationship between expansion of the separation system and medicine costs. This finding indicates that the separation system in Japan might reduce daily medicine costs...
...enables doctors to refrain from prescribing specific medicines, as they are no longer personally interested in drug-related profit margins for their institutions or themselves....
...The magnitude of the partial correlation coefficient for the generic medicine replacement ratio was similar to that of the expansion rate....
記住呢個study地點係日本
醫藥分家 - 3
英國
[3]Dispensing physicians and prescribing pharmacists: economic considerations for the UK.
。。。冇$買
Physician dispensing can benefit patients via savings in time and the monetary cost of visiting a pharmacist, but it restrict drug choice, can compromise safety, and encourages overprescribing except for physicians with drugs budgets.
The effects of physician dispensing on government costs are not yet clear. Over-the-counter (OTC) purchase can save patients the cost of a physician visit and reduce drug costs to some patients, but it can also provide an incentive to pharmacists to profit twice from a drug, at government expense. Switching drugs from prescription-only to OTC reduces the government drug bill, but provides an incentive to pharmacists to overprescribe, and may not be as safe for patients .
Liberalising prescribing by doctors would discourage community pharmacies which provide an advisory service to patients. Liberalising OTC switches would reduce opportunistic assessment of patients by doctors and could compromise patient safety. Separation of physician and pharmacist functions is probably safer for patients. It is concluded that the current situation in the UK, whereby most dispensing is done by pharmacists, is the preferred option other than for those patients who do not live within easy access of a pharmacy. A reassessment of the legal status of drugs and subsequent OTC switch of drugs used to treat minor self-limiting illnesses is also favoured.
補充
1. 香港周街都係藥房.
2. 長時間冇得發揮會唔會失去左counselling 技能?
英國
[3]Dispensing physicians and prescribing pharmacists: economic considerations for the UK.
。。。冇$買
Physician dispensing can benefit patients via savings in time and the monetary cost of visiting a pharmacist, but it restrict drug choice, can compromise safety, and encourages overprescribing except for physicians with drugs budgets.
The effects of physician dispensing on government costs are not yet clear. Over-the-counter (OTC) purchase can save patients the cost of a physician visit and reduce drug costs to some patients, but it can also provide an incentive to pharmacists to profit twice from a drug, at government expense. Switching drugs from prescription-only to OTC reduces the government drug bill, but provides an incentive to pharmacists to overprescribe, and may not be as safe for patients
. Liberalising prescribing by doctors would discourage community pharmacies which provide an advisory service to patients. Liberalising OTC switches would reduce opportunistic assessment of patients by doctors and could compromise patient safety. Separation of physician and pharmacist functions is probably safer for patients. It is concluded that the current situation in the UK, whereby most dispensing is done by pharmacists, is the preferred option other than for those patients who do not live within easy access of a pharmacy. A reassessment of the legal status of drugs and subsequent OTC switch of drugs used to treat minor self-limiting illnesses is also favoured.
補充
1. 香港周街都係藥房.
2. 長時間冇得發揮會唔會失去左counselling 技能?
醫藥分家 - 4
連登仔最愛的台灣
[4]Impact of separating drug prescribing and dispensing on
provider behaviour: Taiwan’s experience
...Combining prescribing and dispensing creates incentives for physicians to increase drug prescriptions and is hypothesized to be a major cause of high drug expenditure and widespread prescription of antibiotics in Asia (Abe 1985;
Yang and Bae 2000). ...
... Several surveys in Hong Kong found that antibiotics were prescribed for approximately 60–80% of cold and flu outpatient visits...
... in an effort to control drug expenditure growth and improve appropriate drug prescription, separating the drug prescribing and dispensing functions of physicians has gained popularity in policy debate among Asian countries....
...In March 1997, Taiwan began implementing a separation policy...
... However, as a result of resistance from physicians, a concession was made whereby clinics with on-site pharmacists were allowed to dispense their own drugs while those without pharmacists were required to use outside pharmacies. ...
...Drug dispensing has been a profitable activity for physicians in Taiwan. ...
... physicians often receive rebates – commonly known as ‘kickbacks’ – from pharmaceutical companies for dispensing certain drugs. ...
... Under this separation policy, physicians are not allowed to dispense drugs (with significant exceptions – see below), thus losing revenue from both the drug reimbursement and the NT$10 (US$0.32) per visit service fee for dispensing.
To compensate for this loss of revenue, the consultation fee for each visit has been increased.
待續
連登仔最愛的台灣
[4]Impact of separating drug prescribing and dispensing on
provider behaviour: Taiwan’s experience
...Combining prescribing and dispensing creates incentives for physicians to increase drug prescriptions and is hypothesized to be a major cause of high drug expenditure and widespread prescription of antibiotics in Asia (Abe 1985;
Yang and Bae 2000). ...
... Several surveys in Hong Kong found that antibiotics were prescribed for approximately 60–80% of cold and flu outpatient visits...
... in an effort to control drug expenditure growth and improve appropriate drug prescription, separating the drug prescribing and dispensing functions of physicians has gained popularity in policy debate among Asian countries....
...In March 1997, Taiwan began implementing a separation policy...
... However, as a result of resistance from physicians, a concession was made whereby clinics with on-site pharmacists were allowed to dispense their own drugs while those without pharmacists were required to use outside pharmacies. ...
...Drug dispensing has been a profitable activity for physicians in Taiwan. ...
... physicians often receive rebates – commonly known as ‘kickbacks’ – from pharmaceutical companies for dispensing certain drugs. ...
... Under this separation policy, physicians are not allowed to dispense drugs (with significant exceptions – see below), thus losing revenue from both the drug reimbursement and the NT$10 (US$0.32) per visit service fee for dispensing.
To compensate for this loss of revenue, the consultation fee for each visit has been increased.
待續
承上
How does the separation policy change physicians’ incentives to dispense drugs?
... their income is positively related to the amount of drugs dispensed
... when physicians are allowed to dispense drugs through on-site pharmacists, they continue to be the residual claimant for drug profit. Thus their income
remains linked to drug dispensing activities and the incentives they face are essentially the same as those faced by physicians in an environment without the separation policy.
Hypothesis 1: impact of the separation policy on drug prescription and expenditure
... suggesting that the separation policy has little impact on drug use. After the implementation of the separation policy, drugs are still prescribed in more than 90% of cases. ...
Hypothesis 3: the impact of separation on total health expenditure
We found that total expenditure per visit did not decrease as a result of the separation policy. Reductions in drug expenditure were compensated by an increase in dispensing service and consultation fees.
How does the separation policy change physicians’ incentives to dispense drugs?
... their income is positively related to the amount of drugs dispensed
... when physicians are allowed to dispense drugs through on-site pharmacists, they continue to be the residual claimant for drug profit. Thus their income
remains linked to drug dispensing activities and the incentives they face are essentially the same as those faced by physicians in an environment without the separation policy.
Hypothesis 1: impact of the separation policy on drug prescription and expenditure
... suggesting that the separation policy has little impact on drug use. After the implementation of the separation policy, drugs are still prescribed in more than 90% of cases. ...
Hypothesis 3: the impact of separation on total health expenditure
We found that total expenditure per visit did not decrease as a result of the separation policy. Reductions in drug expenditure were compensated by an increase in dispensing service and consultation fees.
醫藥分家 - 5
南韓
[5]Consumption of pharmaceutical drugs in exception region of separation for drug prescribing and dispensing program in South Korea
In the year 2000, the South Korean government introduced a program for separation of drug prescribing and dispensing.
The goals of the program are to reduce misuse of drugs and to contain drug expenditures.... reduce the inconvenience for people who reside in areas with a shortage of health care resources.
...many adverse events related to drug misuse occurred in these exception regions after the program reforms were introduced.
...Before the program was introduced, individual physicians and pharmacists could both prescribe and dispense drugs, which was a system that resulted in an inefficient treatment for the patient. ...
不過驚乜丫,萬寧,屈人寺,藥房,通街都係啦。
南韓
[5]Consumption of pharmaceutical drugs in exception region of separation for drug prescribing and dispensing program in South Korea
In the year 2000, the South Korean government introduced a program for separation of drug prescribing and dispensing.
The goals of the program are to reduce misuse of drugs and to contain drug expenditures.... reduce the inconvenience for people who reside in areas with a shortage of health care resources.
...many adverse events related to drug misuse occurred in these exception regions after the program reforms were introduced.
...Before the program was introduced, individual physicians and pharmacists could both prescribe and dispense drugs, which was a system that resulted in an inefficient treatment for the patient. ...
不過驚乜丫,萬寧,屈人寺,藥房,通街都係啦。
醫藥分家 - 6
馬來西亞
[6]Separation of prescribing and dispensing in Malaysia: A summary of arguments
... the transition has been slow due in part to the nonexistence of a dispensing separation policy between pharmacists and medical doctors in private
community practices....
... diluting the role of community pharmacists because of overlapping roles...
... In some countries, particularly in Asia, where pharmacists are lacking and the practice of medicine was traditionally played by a single healer, doctors are still legally allowed to prescribe and dispense medicine. Pharmacists soon found themselves overtrained and underutilized ...
...
Irrational prescribing not only increases treatment cost but also could compromise patient safety and reduce therapy effectiveness....
... dispensing doctors are much less likely to prescribe generic medications compared with nondispensing doctors.10 Overprescribing also could harm patients by introducing hazardous interactions with other medications or with a comorbid illness.
... Separation of the prescribing and dispensing functions would avoid the conflicting roles of physicians who have the potential to profit from the prescription and sale of drugs, and it would introduce a check-and-balance system to prevent such overprescribing practices...
The second rationale for a dispensing separation is the potential high rate of medication errors by physicians, which are highly problematic if left unchecked...
Medical and medicine knowledge has evolved rapidly with new discoveries, and the complex task of prescribing and dispensing cannot be managed by 1 individual. The task should be managed by 2 independent professions....
... A medication expert, or pharmacist, is needed for proper medicine monitoring and dispensing. Holding both roles would not only compromise
the quality expected from each task but also could lead to potential error. (聽講呢排有人因為食錯藥要換肝 ) Evidence points to a 30% smaller duration of medical consultation in dispensing doctor compared with nondispensing doctor practices.....
馬來西亞
[6]Separation of prescribing and dispensing in Malaysia: A summary of arguments
... the transition has been slow due in part to the nonexistence of a dispensing separation policy between pharmacists and medical doctors in private
community practices....
... diluting the role of community pharmacists because of overlapping roles...
... In some countries, particularly in Asia, where pharmacists are lacking and the practice of medicine was traditionally played by a single healer, doctors are still legally allowed to prescribe and dispense medicine. Pharmacists soon found themselves overtrained and underutilized
...Irrational prescribing not only increases treatment cost but also could compromise patient safety and reduce therapy effectiveness....
... dispensing doctors are much less likely to prescribe generic medications compared with nondispensing doctors.10 Overprescribing also could harm patients by introducing hazardous interactions with other medications or with a comorbid illness.
... Separation of the prescribing and dispensing functions would avoid the conflicting roles of physicians who have the potential to profit from the prescription and sale of drugs, and it would introduce a check-and-balance system to prevent such overprescribing practices...
The second rationale for a dispensing separation is the potential high rate of medication errors by physicians, which are highly problematic if left unchecked...
Medical and medicine knowledge has evolved rapidly with new discoveries, and the complex task of prescribing and dispensing cannot be managed by 1 individual. The task should be managed by 2 independent professions....
... A medication expert, or pharmacist, is needed for proper medicine monitoring and dispensing. Holding both roles would not only compromise
the quality expected from each task but also could lead to potential error. (聽講呢排有人因為食錯藥要換肝
) Evidence points to a 30% smaller duration of medical consultation in dispensing doctor compared with nondispensing doctor practices.....無知一問
香港藥劑師可唔可以prescribe 藥物?
香港藥劑師可唔可以prescribe 藥物?
無知一問
香港藥劑師可唔可以prescribe 藥物?
我唔係香港,唔知香港個regulation係點
醫藥分家 – 總結
1醫藥分家帶出來的經濟改變不易測量,但睇落係幫到政府/病人慳到Dge。
2其中一樣減輕帶人負擔的做法就賣dispense generic medicine
3醫藥分家帶出來的效果除左錢之外,仲有分薄左醫生的職能(即係降底medication errors)。
4藥學生要讀GE野多數都係多鳩餘。即係咁,賭波不睇波,賭來幹什麼?
1醫藥分家帶出來的經濟改變不易測量,但睇落係幫到政府/病人慳到Dge。
2其中一樣減輕帶人負擔的做法就賣dispense generic medicine
3醫藥分家帶出來的效果除左錢之外,仲有分薄左醫生的職能(即係降底medication errors)。
4藥學生要讀GE野多數都係多鳩餘。即係咁,賭波不睇波,賭來幹什麼?
醫藥分家 – 總結
1醫藥分家帶出來的經濟改變不易測量,但睇落係幫到政府/病人慳到Dge。
2其中一樣減輕帶人負擔的做法就賣dispense generic medicine
3醫藥分家帶出來的效果除左錢之外,仲有分薄左醫生的職能(即係降底medication errors)。
4藥學生要讀GE野多數都係多鳩餘。即係咁,賭波不睇波,賭來幹什麼?
我覺得如果唔分咁你要pharm做乜
唔計ha入面自己行醫藥分家
你出面唔分既話大部分藥房藥劑師讀完書唯一既作用就係簽紙攞藥
簡直浪費資源
。衍生ge問題多,好似上次HEP. B出事,幫病人出藥之前藥劑師可以check返藥單,減低drug-related problem (DRP).
其實醫生睇epr 都check 到 係醫生自己冇睇到姐
其實醫生睇epr 都check 到 係醫生自己冇睇到姐
香港係大醫生主義
其他HCP 都係輔助角色 做乜都要Consult 醫生 所以冇可能分到家
藥劑師更加冇可能落到Primary care 做簡單 diagnosis 嘅role dispense 某d藥比小病patient 而市民都唔會信藥劑師同醫生一樣專業
而且一改醫藥分家會影響到好多利益關係 香港醫生話語權咁大 冇可能推到
香港人只可以成為部分獸醫亂開藥賺外快嘅犧牲品 我試過初起感冒都開5日抗生素/"特效藥" 比我 為就係為claim爆我份醫療保
呢d事係英國唔會發生 醫生同藥廠冇直接利益關係 所以好少亂開藥 藥劑師都會係Frontline 做你所講嘅audit prescription 同做簡單 consultation 醫小病
香港FF下好
其他HCP 都係輔助角色 做乜都要Consult 醫生 所以冇可能分到家
藥劑師更加冇可能落到Primary care 做簡單 diagnosis 嘅role dispense 某d藥比小病patient 而市民都唔會信藥劑師同醫生一樣專業
而且一改醫藥分家會影響到好多利益關係 香港醫生話語權咁大 冇可能推到
香港人只可以成為部分獸醫亂開藥賺外快嘅犧牲品 我試過初起感冒都開5日抗生素/"特效藥" 比我 為就係為claim爆我份醫療保
呢d事係英國唔會發生 醫生同藥廠冇直接利益關係 所以好少亂開藥 藥劑師都會係Frontline 做你所講嘅audit prescription 同做簡單 consultation 醫小病
香港FF下好
醫藥分家 – 總結
1醫藥分家帶出來的經濟改變不易測量,但睇落係幫到政府/病人慳到Dge。
2其中一樣減輕帶人負擔的做法就賣dispense generic medicine
3醫藥分家帶出來的效果除左錢之外,仲有分薄左醫生的職能(即係降底medication errors)。
4藥學生要讀GE野多數都係多鳩餘。即係咁,賭波不睇波,賭來幹什麼?
我覺得如果唔分咁你要pharm做乜
唔計ha入面自己行醫藥分家
你出面唔分既話大部分藥房藥劑師讀完書唯一既作用就係簽紙攞藥
簡直浪費資源
呢個就係問題之一
//你要pharm做乜//
所以醫藥分家係大TOPIC其中之一,其他功能我慢慢再打啦
WHO話過建議藥劑師比例為1:2000,問題係香港有位塞咁多咩?有空間俾藥劑師發揮咩?簡直浪費資源
。衍生ge問題多,好似上次HEP. B出事,幫病人出藥之前藥劑師可以check返藥單,減低drug-related problem (DRP).
其實醫生睇epr 都check 到 係醫生自己冇睇到姐
咁你都識講醫生自己冇睇啦,呢個咪prevetable me囉
香港係大醫生主義
其他HCP 都係輔助角色 做乜都要Consult 醫生 所以冇可能分到家
藥劑師更加冇可能落到Primary care 做簡單 diagnosis 嘅role dispense 某d藥比小病patient 而市民都唔會信藥劑師同醫生一樣專業
而且一改醫藥分家會影響到好多利益關係 香港醫生話語權咁大 冇可能推到
香港人只可以成為部分獸醫亂開藥賺外快嘅犧牲品 我試過初起感冒都開5日抗生素/"特效藥" 比我 為就係為claim爆我份醫療保
呢d事係英國唔會發生 醫生同藥廠冇直接利益關係 所以好少亂開藥 藥劑師都會係Frontline 做你所講嘅audit prescription 同做簡單 consultation 醫小病
香港FF下好
所以我上面有quote到醫藥學生的能力比較,但記住呢個只係學生比較,出到黎做的差異我反而冇去搵。不過都可以EXPECT到你exposure越多,對果方面的認知越深,個disparity logically gap得越多。
藥劑係有讀primary care,問題時間都係錢,你有幾多時間去screen到人?
另外一樣你有對提的係普羅對藥劑師的印象係點,呢個我諗住稍後再打,要溫書好少時間呻
//醫生同藥廠冇直接利益關係//
笑下算啦 詳情睇上面D literature.
笑下算啦
詳情睇上面D literature.香港係大醫生主義
其他HCP 都係輔助角色 做乜都要Consult 醫生 所以冇可能分到家
藥劑師更加冇可能落到Primary care 做簡單 diagnosis 嘅role dispense 某d藥比小病patient 而市民都唔會信藥劑師同醫生一樣專業
而且一改醫藥分家會影響到好多利益關係 香港醫生話語權咁大 冇可能推到
香港人只可以成為部分獸醫亂開藥賺外快嘅犧牲品 我試過初起感冒都開5日抗生素/"特效藥" 比我 為就係為claim爆我份醫療保
呢d事係英國唔會發生 醫生同藥廠冇直接利益關係 所以好少亂開藥 藥劑師都會係Frontline 做你所講嘅audit prescription 同做簡單 consultation 醫小病
香港FF下好
所以我上面有quote到醫藥學生的能力比較,但記住呢個只係學生比較,出到黎做的差異我反而冇去搵。不過都可以EXPECT到你exposure越多,對果方面的認知越深,個disparity logically gap得越多。
藥劑係有讀primary care,問題時間都係錢,你有幾多時間去screen到人?
另外一樣你有對提的係普羅對藥劑師的印象係點,呢個我諗住稍後再打,要溫書好少時間呻
我都溫緊書回你 樓豬加油
